
This is a complex condition where the patella (kneecap) repeatedly slips out of position fully (dislocation) or partially (subluxation). This normally happens towards the outside of the knee (laterally).
When this happens for the first time it is usually trauma related and requires a violent force. If it occurs repeatedly, less force may be required each time; the risk of recurrence is moderate to high depending on numerous patient factors and index injury severity.
If this happens on a repeated basis, it is not only disabling at the time of injury and for the period after as the injured tissues heal, but concomitant articular cartilage damage (patello-femoral joint) can occur as a process of attrition, complicating management of the condition and potentially giving rise to chronic discomfort.
It is important to understand why this has happened in your particular case. There are several important patient related factors to be aware of which may apply to you and thus, together with acute injury patterns or chronic injury related changes, may dictate further management.
As aforementioned, there are many factors to address to achieve patella stability. Treatment starts with a tailored physiotherapy program and often forms the mainstay of preventative treatment strategies. otherapy, instability still occurs, surgical reconstruction may be of value.
Generally, the need for acute surgery (i.e. immediately after a dislocation) is only recommended if swelling of the knee joint needs to be relieved or a loose fragment of cartilage/bone needs to be removed. This can be done by knee arthroscopy.
In view of the large spectrum of injury and symptomology that patella instability encompasses, not to mention the numerous individual patient factors and expectations that accompany any medical condition, Mr Patel prefers to discuss your particular case with you in detail and plan the management accordingly after thorough assessment and investigation.
It is likely that X-rays and MRI will be requested for most knee injuries. Please see Surgery FAQs to see if you will need any other tests e.g. blood tests before your surgery.
Surgery for patella instability involves both arthroscopy and open surgery. The main areas addressed are:
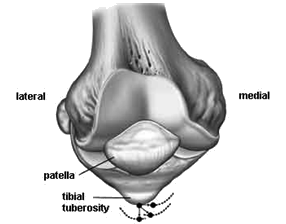
How the patella sits it may tilted to one side (lateral) or naturally sit towards the outer aspect of the joint, which predisposes it to slipping out of place. This can be corrected. Or it can sit too high (patella alta) and thus needs to be brough down to sit correctly (tibial tubercle distalisation).
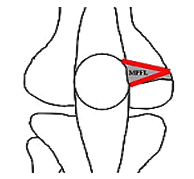
There are stabilising ligaments, the most important one of which is on the inner aspect of the knee between the patella and the end of the femur (thigh bone). It is called the medial patello-femoral ligament (MPFL) this may be reconstructed using a donor tendon.
The articular cartilage on the under surface of the patella may have become damaged with repeated episodes of instability. The damage can be assessed and if necessary treated to either stabilise the lesion, for example in the case of a flap injury, or if deemed appropriate, a cartilage regeneration technique e.g. microfracture may be performed. If the damage is extensive then another option may be to offload the worn area. This can be achieved by a tibial tubercle transfer (osteotomy), which can also positively affect the dynamic position of the patella (i.e. when the quadriceps muscles are active) to ensure greater stability. Finally the groove (trochlear groove) that the patella sits in may be too shallow and a procedure called a trochleoplasty can be performed to deepen the groove and thereby improve stability. Mr Patel is one of only a few surgeons with good experience in this latter surgery.
Not all the areas above may need to be addressed and thus any combination of techniques may be utilised.
Patella instability surgery is complex. Each individual case requires careful planning. It usually involves a short hospital stay post-operatively and extensive rehabilitation programs to ensure success. A knee brace is commonly used initially (up to 12 weeks) to control knee motion and allow healing, but this may be shorter depending on the surgery carried out.
Surgical techniques, outcomes and potential complications are best discussed with Mr Patel in person.
Please visit www.orthopedia.com for more information

